2015 is set to be a progressive year for eHealth. Following the momentum built up in 2014, I take a look at the top 4 predictions and eHealth “hot-spots” that deserve the attention of Healthcare strategists in 2015.
Personally Controlled Electronic Healthcare Record (PCEHR)
In 2015 expect to see substantial progress in the PCEHR and integration of clinical information. Some of the progress made in 2014 will flow on to impact providers and consumers of Healthcare in 2015. Healthcare providers in particular should already have plans in place to align with the work NEHTA is doing, and if not, get prepared now for change.
The National E-Health Transition Authority (NEHTA) will offer funding to private hospital groups to begin integrating their systems with the PCEHR. They have released the details of their Private Hospital PCEHR Rapid Implementation Program (RIP), which will contribute towards the technical requirements for uploading and viewing of clinical documents. Release five of the PCEHR will pave the way for NEHTA to work with pathology and diagnostic imaging services to enable provider information systems to send PDF pathology and diagnostic imaging report to the PCEHR.
In Aged Care, 2015 will (hopefully) see the formation of a single client record that aligns the Aged Care Gateway system and the central client record, to the PCEHR.
In Melbourne, Western Health is gearing up to enter phase two of a project to securely deliver notifications from its hospital systems directly into GP desktop practice management software through an SMD-compliant eMessaging Gateway. This initiative, and others like it, will become more common-place in 2015.
Expanding Consumer Choice
Consumer Directed Care (CDC) is set to be more widely integrated in 2015, with a broadening of services offered under this model. Whilst CDC within the home and community care setting will continue to develop strengthen, residential aged care looks to embrace the same model of handing control to consumers over their choice of providers.
The My Aged Care gateway website for example, could be the “virtual marketplace where consumers and providers – or demand and supply – meet”. The quote from a speech delivered by Senator Mitch Fifield goes on to say “Trip Advisor style capacities on the My Aged Care website will develop ratings for the quality of providers and their services, according to what matters to consumers, rather than what Departments and providers think they should be”.
CDC for Residential Aged Care is good for consumers, and is currently in the mindset of policy makers. Residential Aged Care providers would be wise to consider the impacts of this, and think about strategies to best position themselves for the years ahead.
A current challenge is how Healthcare Providers will manage the new CDC reporting requirements. From July 2015 all Home Care Packages will be delivered on a CDC basis, so there is some concern in the industry around the lack of IT capability to deliver on these reporting requirements as July 2015 approaches.
Digital Healthcare
In 2015 many facets of healthcare will increasingly be digitised. Healthcare digitisation offers many benefits around clinical workflow automation, storage savings, longevity of records, and transmission and communication of clinical information.
Fully digital hospitals promise connection, integration and digitisation of medical records, x-rays, pathology results, radiology imaging, medications, CT/MRI scans, vital signs and other health information. Digitisation also provides opportunities around big data analytics and business intelligence to gain a broader picture of patients to improve health outcomes.
Other examples of digital healthcare include: doctors using speech recognition software to translate voice instructions directly onto patient records; linking patient meal planning with allergies and conditions (eg diabetes); medication verification and stock supply; and fingerprint biometrics for clinical staff access to rooms and systems.
It is not just hospitals that will benefit from digital healthcare in 2015. In the home care space a clinically validated monitor has recently been released that allows home users to measure blood pressure and heart rate, and connect it wirelessly to a mobile app. QardioArm works with Apple’s HealthKit, which lets users access all their health and wellness information in one place. It also records irregular heart beat history to provide a reference for doctors. This is just one of many examples.
With digitisation of healthcare inevitably on the rise, appropriate management and governance within this new paradigm will be required. One example that helps pave the way is the release of the “Clinical Images and the Use of Personal Mobile Devices” guide, which was created to assist doctors and medical students in the proper use of personal devices such as smartphones, when taking and transmitting clinical images.
Interoperability
Interoperability is essentially an expansion of the PCEHR.
In the medication management space, 2015 may be the year to directly import medication information out of the PCEHR or GP systems straight into Healthcare Providers medication management (or clinical) system. From a hospital perspective, work needs to be done to address the challenges faced by interoperability between different clinical systems, as well as the challenges in mapping the Australian Medicines Terminology (AMT) to SNOMED CT-AU.
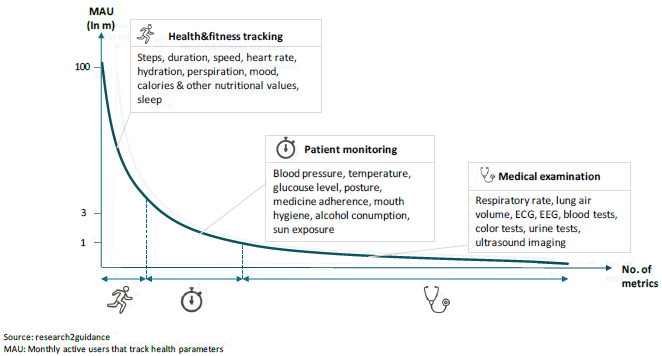
2015 will also see the continued proliferation of wearable devices. A recent survey from Kronos indicates that 30 per cent of Australians use wearable devices in their personal lives. This adoption rate could result in a smooth transition to wearables for health and fitness use. Health and fitness data can be useful in doctor consultations to aid diagnostics, and in the future could be designed as medical devices and for monitoring general health and well-being. There will be a time where the patient will upload the data and it will end up on the health professional’s screen. It may not happen in 2015, but it will happen.
Some wearable devices that already exist include glucose meters that allow clinic alerts and remote monitoring; devices that monitor vital signs; devices and apps that allow patients to monitor their diets; and apps to help with medication compliance. Check out my blog “The Mobile eHealth Revolution” for more information.